Views/Visit: 646
Case 47: Infant presented with shortness of breath and dysphagia.
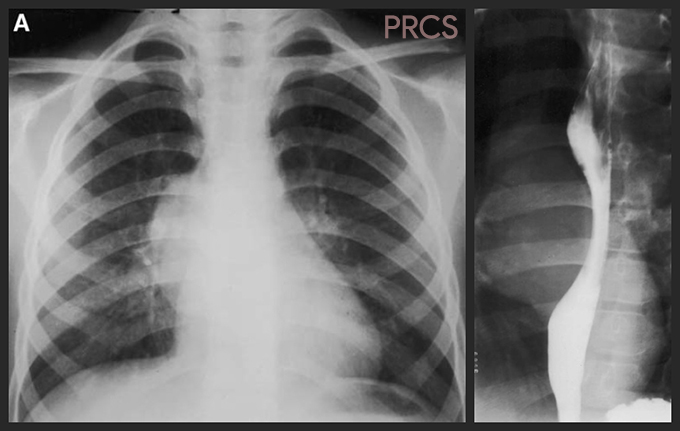
Case: Infant presented with shortness of breath and dysphagia. There is posterior mediastinal mass lesion projecting to the right of spine.
Q: What is the most likely impression?
Answer : Bronchopulmonary foregut malformation.
Details : upper GI study shows the mass narrowing the esophageal lumen. Surgical proved to be a spherical esophageal duplication cyst.
BPFM (Bronchopulmonary Foregut Malformation) encompasses spectrum of developmental abnormalities derived from the embryonic foregut, such as Duplication cysts arising anywhere from the pharynx to the duodenum, neurenteric cysts, bronchogenic cysts, pulmonary sequestrations, and occasionally CPAM and CLE.
Esophageal duplication cysts (EDCs) are the second most frequent type of enteric duplication (after ileal) accounting for 15% to 20% of cases. Pathologically, they have a well-developed coat of smooth muscle and are lined by epithelium derived from some portion of the alimentary tract. Most lie adjacent to the wall of the esophagus or are intramural, but extraluminal. Gastrointestinal tract duplications may be either spherical or tubular in shape. Patients may be asymptomatic, with the cyst being discovered incidentally when they are imaged for some other indication. Alternatively, they may present with acute or subacute symptoms, the nature of which depend on the anatomic location of the cyst, the mass effect it causes, or complications related to the cyst lining.
Approximately 60% of EDCs are located in the distal third of the esophagus, 17% are in the middle third, and 23% are at the cervical level. The more distal the location, the more likely the cyst is to be asymptomatic. Cervical EDCs may present as a painless enlarging neck mass or with symptoms of upper airway obstruction. EDCs located in the middle third of the esophagus are more likely to cause airway obstruction leading to cough, wheeze, shortness of breath, and recurrent infection. Impingement on the adjacent esophagus can cause dysphagia, vomiting, or feeding intolerance. Over 40% of EDCs are lined by gastric mucosa; this can bleed or ulcerate. Ulceration may cause the cyst to perforate into the adjacent airway or esophagus causing hemoptysis or hematemesis.
A mediastinal EDC lies posteriorly on the lateral chest radiograph. The cysts are well-demarcated and usually of soft tissue density. Cervical EDCs may be examined using US, when a cystic lesion lined by an echo-bright mucosal layer is seen. A barium swallow study either shows the esophagus deviated to one side by the cyst or an intramural, extraluminal filling defect.
Reference : Anne Paterson. Imaging evaluation of congenital lung abnormalities in infants and children. Radiol Clin N Am. 2005; 43: 303-323